





.jpg)
.png)










A patient recently told me the story of her statin-intolerant sister, who was referred to a cardiologist she had seen for chest pain a few years earlier. When he entered the room, she explained that she could hardly walk or even get out of bed on atorvastatin. The doctor simply stated there was nothing he could do for her and walked out, leaving her confused and hurt. We can do something for these patients and it starts with listening.
Statin clinical trials suggest an incidence of adverse muscular events of ~ 1.5 - 3%, but the true incidence of statin intolerance (SI) is likely between 10% and 15%.1, 2 In a recent one-month chart review of 393 patients seen in our lipid clinic, 185 (47%) were originally seen for statinrelated adverse events, and 145 (37%) of these had a history of SI related solely to musculoskeletal complaints.
So, what can we do for these patients? Of the 145 SI patients from our review, 90% (129 patients) are actually on a statin today – 14% on a statin alone and 83% on statins dosed at very low doses and/or dosed 2-4 times weekly, in combination with other lipid lowering medications. The average low-density lipoprotein (LDL) reduction in these patients was 50.8%. So the crux of therapy for our statin-intolerant patients is STATIN, but often dosed in an unconventional manner in unusual combinations with other lipid-lowering agents.
Following is our approach to the SI patient.
First, listen to the patient. Just listening with a compassionate ear will make the patient more receptive to at least try another statin at a very low dose.
Second, educate the patient on the benefits of statin therapy. The patient’s perception of these drugs often comes from the evening news, a friend’s report of some statin horror story or the hungry lawyer ads on T.V. They rarely hear the good news. A favorite “one-liner” for this purpose: “For every one high-risk person on statin who has died from an adverse muscle event, 1,188 people DIDN’T DIE because they took their statin,” a calculation based on the incidence of fatal rhabdomyolysis of 0.3/100,000 personyears of statin therapy3 compared to the 360 lives saved per 100,000 personyears of statin therapy in 17 secondary prevention trials. A little pain is worth a lot of gain.
Third, rule out other causes of myopathy and evaluate potential exacerbating factors by checking a TSH, B12, vitamin D level. A baseline CK should be established and monitored with symptoms as recommended by the National Lipid Association Statin Safety Task Force.3
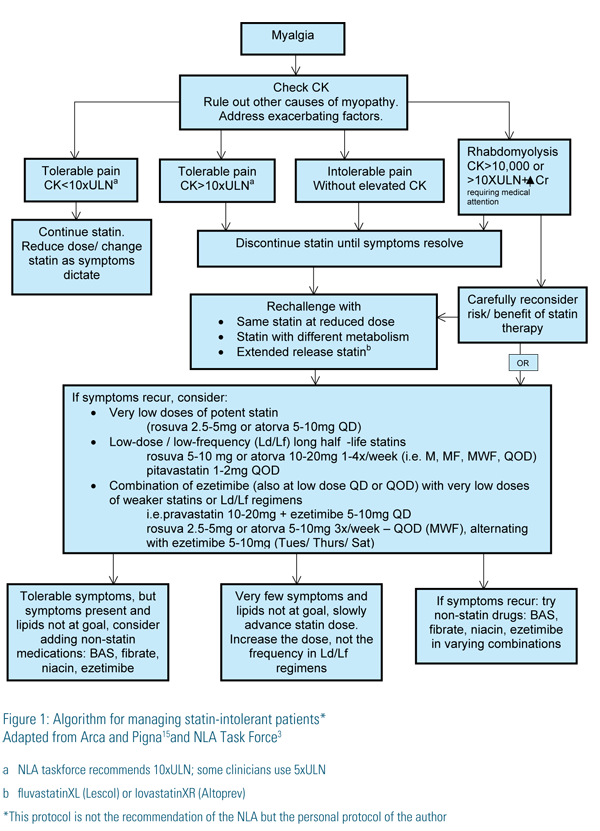
Finally, we initiate drug therapy by:
(1) Switching to another statin, one with a different metabolism or to an extendedrelease preparation (fluvastatinXL or lovastatin XR-Altoprev).
(2) Initiating very low doses (Ld) of long half-life statins at a low frequency (Lf), i.e. once a week to every other day (QOD), using primarily rosuvastatin (19 hours) and atorvastatin (14 hours) or pitavastatin (11 hours) QOD.
(3) Combining very low daily doses of weaker statins or alternate-day dosing of long half-life statins with ezetimibe – also used at a low-dose/low-frequency (5-10mg daily, QOD or 3 times weekly) – for reduced symptoms, lower cost or if full doses cause a reduction in high-density lipoprotein (HDL).
(4) Combining the above (statin +/- ezetimibe) or ezetimibe alone with other non-statin lipid-lowering medications (BAS, niacin, fibrates) with an intense effort to choose a drug that has some clinical trial evidence of benefit for that individual patient, i.e. fibrate for triglycerides>200mg/dl and HDL<40mg/ dl, colesevelam for diabetics with close triglyceride monitoring, niacin for LDLs not at goal and NOT for those with severe expressions of metabolic syndrome, monitoring platelets and symptoms of ulcers and gout.
Since most patients referred to lipid clinics have already failed multiple attempts with multiple statins, proceeding directly to options 2 and 3 above is reasonable. We almost always start with rosuvastatin 2.5mg -5mg, taken on Mondays, Wednesdays and Fridays (MWF), with directions to add ezetimibe 5mg (1/2 10mg pill) on Tuesdays, Thursdays and Saturdays (TuThSa). Providing samples for this first cycle definitely improves compliance. A normal week’s supply lasts a month with the pill splitting and QOD dosing. We repeat labs after six weeks. Once the patients see the usually significant improvements, they are encouraged enough to continue and even increase the medications. We advance the statin very gradually, as tolerated, by increasing the dose first, not the frequency. For insurance purposes, we often switch to atorvastatin 5-10mg dosed at the same frequency or change to very low doses of weaker statins (i.e. pravastatin 10-20mg) daily. From there, it’s a slow process of tweaking, determined by other lipid abnormalities, comorbidities and cost.
Following is a summary of studies evaluating the efficacy and tolerability of low-dose/low-frequency (Ld/Lf) dosing strategies with statins:
(1) Piamsomboon et al.4—In 61 patients treated with atorvastatin 10mg QOD, LDL was reduced 30%.
(2) Juszczyk et al.5—In 25 patients treated with atorvastatin QOD (mean dose 18.8mg) or rosuvastatin QOD (mean dose 9.7mg), LDL reductions were 43% and 28%, respectively.
(3) Wongwiwatthanaukit et al.6—In 81 patients treated with rosuvastatin 10mg qd vs. QOD, LDLs were reduced 48% and 39%, respectively, and 85% vs 70% achieved NCEP targets, neither statistically significantly different.
(4) Jafari et al.7—In 54 patients, there were no statistically significant differences in LDL reductions between atorvastatin dosed at 10mg qd, 10mg QOD or 20mg QOD after 6 weeks of treatment; all tolerated treatment.
(5) Keles et al.8—In 61 patients treated with atorvastatin 20mg qd vs QOD, there was no significant differences in the reductions of LDL or hsCRP after 3 months.

Similar trials performed in STATIN INTOLERANT patients include:
(1) Backes, et al.9—In 51 patients treated with rosuvastatin 2.5-10mg QOD, (mean dose 5.6mg), LDL was reduced 34.5%, 50% achieved National Cholesterol Education Program goals and 72.5% tolerated therapy.
(2) Gardala, et al.10—In 40 lipid patients receiving rosuvastatin 5-10mg twice weekly (Mondays and Thursdays); LDLs were reduced 26% and 80% tolerated treatment.
(3) Rusinger, et al.11—50 patients receiving rosuvastatin 2.5-20mg once a week; LDLs were reduced 23%, 74% tolerated treatment, but only 27% reached their NCEP goal.
Studies evaluating Ld/Lf or extended release statin therapy in SI patients in combination with ezetimibe include:
(1) Athyros, et al.12—In 54 patients receiving ezetimibe 10mg QD for three months and subsequently receiving atorvastatin 10mg twice weekly for three months, LDLs were reduced 34%, 84% achieved LDL goals vs. only 9% on ezetimibe alone, and only one patient could not tolerate the addition of atorvastatin.
(2) Reddy, et al.13—In 23 patients intolerant of atorvastatin or rosuvastatin receiving the same drug dosed twice weekly plus ezetimibe twice weekly plus colesevalam 6 pills a day, LDLs were maintained at the level produced by daily dosing, but 87% of patients tolerated treatment, and HDLs went up in the rosuvastatin patients.
(3) Stein, et al.14—In patients receiving daily fluvastatin XL 80mg, ezetimibe 10mg or both, LDLs were reduced 33%, 16% and 41%, NCEP targets were achieved in 59%, 29% and 84%, and muscle-related side effects occurred in 17%, 24% and 14%, respectively.
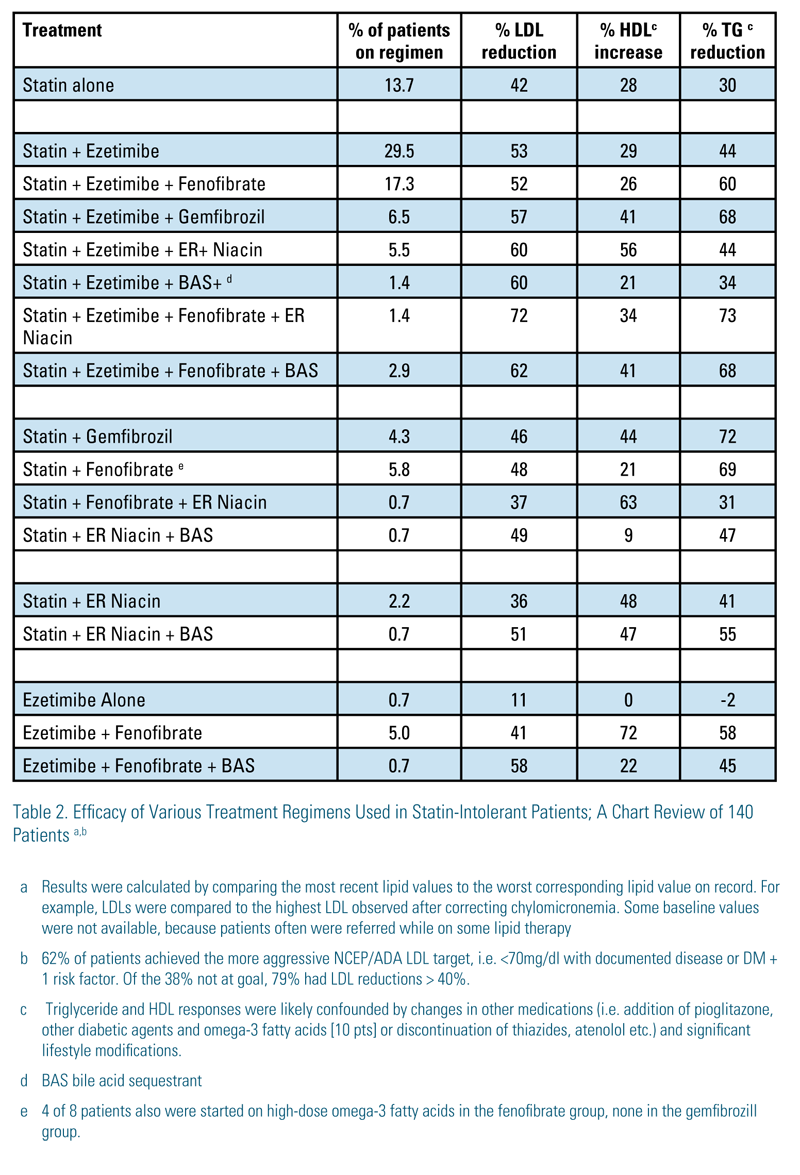
Results from our chart review are consistent with the above reports: 29 of 140 SI patients were on non-daily doses of statins, and 44 were on statin in combination with ezetimibe alone with an average LDL reduction of 52%. Many of these were on non-daily low doses of ezetimibe (5mg 2-4 times per week). An additional 33 patients were on statin+ezetimibe+other non-statin drugs and had an average LDL reduction of 62%. Coincidentally, 62% of the patients were below the more aggressive NCEP targets; 79% of those not at goal had >40% LDL reductions.
Following statins and ezetimibe, fibrates were the drugs used at the next highest frequency. This is not surprising, because 295 of 393 (75%) of our patients had TGs >200, and 22% were referred with severe hypertrigyceridemia (TG>500). Even so, less than half of these patients were on full-dose fenofibrate. Fenofibrate can help lower the LDL further and often results in a dramatic LDL reduction when combined with ezetimibe alone, a very consistent finding in the completely statin-intolerant patient. If fenofibrate lowers HDL and increases creatinine, especially enough to preclude the use of metformin, we reduce the dose or stop it. Table 1 summarizes the drugs used and Table 2 the lipid values achieved with various drug combinations. Only 20% of the patients were on a Ld/ Lf statin-dosing schedule, but most were originally started on rosuvastatin (2.5mg) three days a week. Most patients tolerate a very gradual increase in the statin dose – to a point. The art is knowing when to stop.
While all of these results of alternate-day statin dosing, especially in combination with other lipid drugs, are quite remarkable and encouraging, these are non-approved strategies and no clinical trial evidence for cardiovascular risk reduction exists. Therefore, these strategies should be reserved for those patients who have failed recurrent attempts of conventionally dosed statins. Designing a clinical trial to evaluate these kinds of treatments in SI patients would be a monumental task. However, if one were designed so medications were meticulously tailored for the individual patient – the way most of us treat these SI patients – compared to those treated with statin alone, these patients just might come out ahead – or at least they could get out of a chair!
Disclosure statement: Dr. Honkanen is on the speaker’s bureau for Merck & Co., Inc., Astra-Zeneca and Amarin Pharma, Inc.
Article By:

Director of The Cholesterol and Lipid Treatment Center
Mobile Diagnostic Center
Providence Hospital
Mobile, AL
Diplomate, American Board of Clinical Lipidology