





.jpg)
.png)










In 2009, a 75-year-old Tsimane man and his wife awoke and went out into the rain forest around their home in the Amazonian lowlands of Bolivia to collect jajata, a palm like plant used to make roofing. Walking home in the afternoon, he collapsed to the ground, unconscious. His wife shook him and after a few minutes he regained consciousness. He complained of chest pain radiating down his left arm. He was having trouble breathing but managed to stand and walk home. He was uncomfortable all night and had trouble breathing. In the morning, his wife found him dead. He represents the only known case of a myocardial infarction recorded in the 16,000-person Tsimane tribe over the last decade. What happens about once a minute in the United States,1 is rare in this culture.
Anthropologists Hillard Kaplan and Michael Gurven of Chapman University and the University of California, Santa Barbara, respectively, have been studying this tribe living an ancient lifestyle for 17 years.2-6 The Tsimane are subsistence farmers. Each family hunts, fishes and farms for their own food. While their children now go to small local schools, the adults typically have less than one year of schooling. Most Tsimane adults are unable read or write. Women give birth to a mean of nine children. They live in villages generally of 50-100 persons in thatched huts or small wooden 1-2 room structures. Cooking is by open fire. While 20% of children die by the age of 15, mostly of infection, the modal age of death is 70 years.7 Most villages hug the Maniqui River, a tributary of the Amazon. Transportation is by walking or by dugout canoe, poling through the water or using a small motor. (Figure 1)

Figure 1. Tsimane man crossing the Maniqui River in a dugout canoe.
The Tsimane serve as a model of how our ancestors lived 200 or so generations ago, prior to humans moving into cities and developing job specialization. Funded by the NIH to study the natural history of aging, as well as other topics, Kaplan and Gurven, created the Tsimane Health and Life History Project (THLHP) research team. Strikingly, they rarely observed clinical evidence of atherosclerosis.4 Examining this further, they teamed up with then University of New Mexico cardiology fellow, Chris Rowan, to perform verbal autopsies. Using World Health Organization methodology, they could only document one death from myocardial infarction, the case described above.
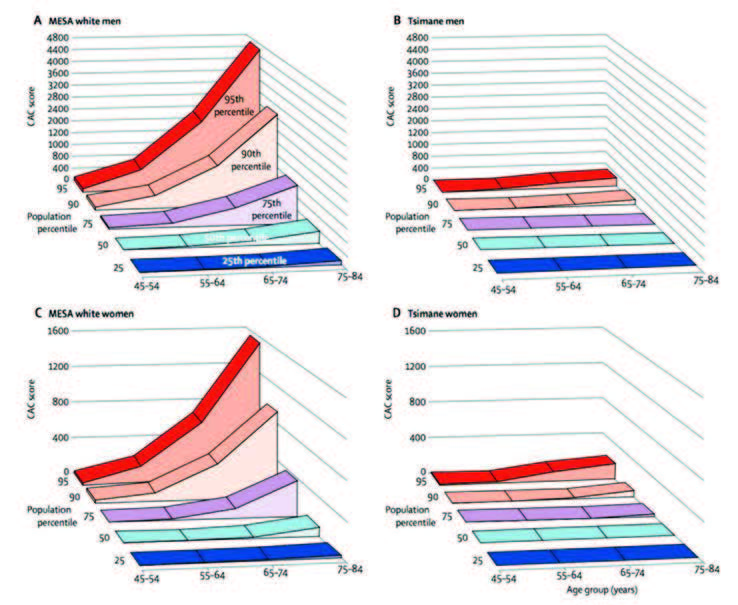
Figure 2. CAC score by age and CAC percentile in MESA white men (A) and Tsimane men and in MESA white women (C) and Tsimane women (D). Adapted with permission from Kaplan H, Thompson RC, Trumble BC, et al. Coronary atherosclerosis in indigenous South American Tsimane: a cross-sectional cohort study. The Lancet. 2017;389(10080):1730-1739.
In the meantime, the Horus mummy research team had been studying ancient mummies since 2008. As reported in JAMA,8JACC Imaging,9 and The Lancet,10 the team found that atherosclerosis was present and common in ancient Egyptians, Peruvians, North American Native Americans, and Aleutian Islanders. The team could not find a culture that did not have atherosclerosis. As the heart typically dissolves over the years after mummification, the atherosclerosis documented was typically of the aorta, carotids, iliacs, and femorals, though several cases of multi-vessel CAD were documented.9-11 The clinicians on this team of cardiologists, radiologists, and other physicians, in addition to anthropologists and biologists, used this information to reassure modern-day patients. Meeting a patient with their first clinical event, such as a myocardial infarction, they urged the patient not to blame themselves for developing atherosclerosis. That atherosclerosis had been documented as long ago as 5,300 years ago in the Tyrolean Iceman12 and was frequent in many ancient cultures. In addition to reassurance, they also informed the patient that we now know of much that can be done to slow down the process with medication and lifestyle changes.

Figure 3. Tsimane man clearing a plot of trees for slash and burn agriculture.
It appeared to the Horus team that atherosclerosis was part of the natural aging process. Despite a mean age of the mummies of only 37 years, atherosclerosis could be documented in one-third of adult mummies studied.10 They could not find a culture free from atherosclerosis.
On the other hand, the experience of the THLHP team was that the Tsimane appeared to live a life without atherosclerosis. Getting together in 2013, the teams began collaborating to examine this apparent paradox. They designed a study that ultimately brought 706 Tsimane aged 40-91 years of age (mean 58 years) out of the rain forest to Trinidad, the capital of the Beni region of Bolivia, where the Tsimane lived, underwent non-contrast CT coronary calcium scoring (CAC) to evaluate for coronary atherosclerosis.7 To the surprise of the Horus team, the average Tsimane lived a life without developing CAC – 85% of the 706 adults had no CAC. Figure 2 shows that the rate of progression of CAC is much slower in Tsimane men and women than in the US MESA cohort. Moderate CAD, as defined by a CAC >100 Agatston Units (AU), occurred in 3% of the Tsimane, about 1/10th of the MESA prevalence. Of the 46 Tsimane aged >75 years (mean 81 years), 65% had no CAC. The mean CAC of this older group was 26 AU. Using MESA as a comparator, 93% of Caucasians in this older age group had CAC, with a mean score of 270 AU. Thus, overall CAC levels were 1 1/10th of what was reported in MESA.

Figure 4. A Tsimane woman preparing a squirrel monkey over an open fire in her home
Why might this have occurred and what lessons does it provide for our patients?
Mean blood pressure of the 706 Tsimane studied was 116/73 mm Hg, mean fasting blood sugar 79 mg/dL, none had a FBS of >126 mg/dL, so none had diabetes, BMI was 24, and lifetime LDL was 71 mg/dL.7 Mean HDL was 38 mg/dl. Smoking was extraordinarily rare and no Tsimane were on lipid lowering or hypertensive medication.

Figure 5. Tsimane woman and child crushing dried corn with large stone.
The lifestyle and diet of the Tsimane are indeed extraordinary. Having to hunt or grow their own food, the Tsimane spend less than 10% of daylight hours sedentary. Converting their accelerometer measured physical activity,13 men averaged 17,000 steps per day and women 16, 000 steps per day.14 This compares to an estimated mean for the US of 6,500 per day. Such an activity level makes the Tsimane lifelong athletes.
Their diet differs based on the village they live in, particularly how close it is to the river, as some live deep in the rain forest. A typical diet measures 17% protein, 67% carbohydrate, and 16% fat, of which 11% is mono or polyunsaturated and 5% saturated. Trans fats consumption is <0.01%. Without stoves or preservatives, their food is unprocessed and is literally farm to open fire to meal. Groups of men typically hunt local animals during the day with shotguns and bow and arrow or fish with arrows, hook and line, and nets. What they bring home is put in a stew of carbohydrates grown from the family farms. Of the protein, one-third to one-half is fish, including catfish and piranha, with the remainder lean game animals, including peccary, tapir, capybara, and monkey. Farm products include plantain, manioc, corn, and rice. The Tsimane gather fruit including mango, papaya, orange, and guineo.

Figure 6. Tsimane thatched roof home and horticultural plot.
Figures 3-6 demonstrate some of their lifestyle activities, chopping down trees for slash and burn agriculture, preparing food and a family home.
Based on the teams’ work with ancient mummies and contemporary hunter-farmers who are alive but live an ancient lifestyle, humans are inherently prone to develop atherosclerosis. However, prevention works, a diet and lifestyle that result in lifetime of remarkably low risk factors can delay or defer coronary atherosclerosis throughout a human lifetime.
Funding sources: NIH R01AG024119-01-08; R01AG054442; National Endowment for the Humanities
Disclosure statement: Dr. Rowan has no disclosures to report. Dr. Thomas has received honorarium from Astellas Pharma and an institutional research grant from Amgen and Novartis.
References available here.
Article By:

Medical Director for Research
Renown Institute for Heart and Vascular Health, Healthy Nevada Project
University of Nevada School of Medicine
Reno, NV

Medical Director
Cardiovascular Program Development
MemorialCare Heart and Vascular Institute
Clinical Professor
Division of Cardiology
University of California, Irvine
Fountain Valley, CA