





.jpg)
.png)










Since loss-of-function mutations in proprotein convertase subtilisin-kexin type 9 (PCSK9) were found to be associated with reduction in low-density lipoprotein cholesterol levels (LDL-C) and coronary events1, there has been great anticipation of the development of effective therapeutic agents to inhibit PCSK9. Two monoclonal antibodies to PCSK9, alirocumab and evolocumab, became commercially available in the U.S. in summer 2015. Evidence of the lipid-lowering efficacy of these agents has been robust2 and evidence of clinical cardiovascular-event reduction has begun to arrive.
Through 2016, the available data included prespecified but exploratory analyses of two open-label randomized extension studies. The OSLER clinical trial program evaluated evolocumab and the ODYSSEY LONG-TERM trial evaluated alirocumab, each studied against a background of statin therapy. Both trials showed a reduced incidence of major cardiovascular events with the active PSCK9 inhibitor therapy, though the total number of events was small.3,4 In both cases, the event reduction was found via post-hoc analysis and neither trial was powered to detect a difference in clinical atherosclerotic cardiovascular disease (ASCVD) events.
In early 2017, we now have the FOURIER trial, a randomized study of the addition of evolocumab, in either of its two clinical dosing regimens (140mg subcutaneous [s.c.] every two weeks or 420mg s.c. monthly) added to a background of optimized statin therapy. The trial was appropriately powered to assess clinical cardiovascular events, with more than 13,000 patients enrolled in each group. Both groups were well-treated by traditional lipid criteria, with a median baseline LDL-C of 92 mg/dl. The addition of evolocumab lowered LDL-C by an additional 59% at 48 weeks with a median on-treatment LDL-C of 30 mg/dl in the active treatment arm. The primary endpoint – a composite of cardiovascular death, myocardial infarction, stroke, hospitalization for unstable angina or coronary revascularization – was reduced by 15% over the median duration of follow-up of 26 months. The prespecified secondary endpoint, the “harder” components of the primary endpoint – a composite of cardiovascular death, myocardial infarction, or stroke – was reduced by 20%. The benefits of evolocumab therapy appeared to increase over time, with a 25% reduction in the secondary endpoint after the first year.5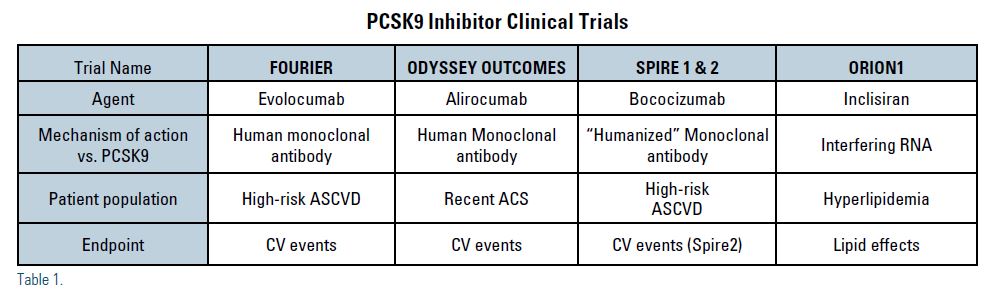
Cardiovascular death was not reduced with evolocumab therapy, however. Cause for concern? Perhaps not. Most cardiovascular-event trials of lipid-lowering therapies have included much longer subject follow-up, around five years. In many of those trials, cardiovascular-death benefit did not emerge until after two years of active treatment.6-12
Early in the PCSK9 clinical trial development programs, some concern arose as to whether the very low on-treatment LDL levels achieved by PCSK9 inhibitor therapy would lead to a decline in neurocognitive function.13 Importantly, in the EBBINGHAUS study, an objective assessment of neurocognitive function in nearly 2,000 patients enrolled in the FOURIER trial, no decline in neurocognitive function was found with evolocumab therapy.14
The FOURIER trial population included patients with clinical atherosclerotic cardiovascular disease and additional characteristics placing them at increased cardiovascular risk. A slightly different patient population is being studied in the ongoing ODYSSEY OUTCOMES trial, a randomized investigation of alirocumab therapy against a background of standard lipid-lowering therapy in reducing major cardiovascular events. Approximately 18,000 patients 4-16 weeks post-acute coronary syndromes have been enrolled and results are anticipated by early 2018.15
A third PCSK9 inhibitor, bococizumab was well into clinical development when its clinical trial program was halted in November 2016 after neutralizing antidrug antibodies developed in a large number of patients and significantly diminished the LDL-lowering effects.16 Unlike the other two available monoclonal antibodies to PCSK9, this agent is not fully “human” but “humanized,” likely explaining the greater propensity for antibody formation. No neutralizing antibodies developed with evolocumab therapy in the FOURIER trial.5
Another mechanism of action of PCSK9 inhibition is in early clinical development. Inclisiran, a small “interfering ribonucleic acid (RNA)” that targets PCSK9 messenger RNA (mRNA), has been shown in a Phase II trial to produce sustained reductions in PCSK9 and LDL-C levels for up to six months with a single subcutaneous injection; greater efficacy is demonstrated if a second injection is administered after 90 days.17 Further investigations are moving forward in the ORION clinical trial program.
In advanced mathematics, Fourier analysis is a method of defining periodic waveforms. We all look forward to catching the periodic waves of PCSK9 clinical outcomes data to come.
Disclosure statement: Dr. Shurmur has spoken for Sanofi Regeneron.
References can be found here.
Article By:

Division Chief, Cardiology
Texas Tech University Health Sciences Center
Lubbock, TX
Diplomate, American Board of Clinical Lipidology