





.jpg)
.png)










Most coronary heart disease occurs in those over the age of 65.1 Statins reduce cardiovascular morbidity and mortality in both primary and secondary prevention. Data from the Cholesterol and Recurrent Events (CARE),2 Long-term Intervention with Pravastatin in Ischemic Disease (LIPID),3 and Scandinavian Simvastatin Survival Study (4S)4 trials have shown statins to be as effective in the elderly as in younger populations.5 The NLA Recommendations for Patient-Centered Management of Dyslipidemia – Part 2 recommends thoughtful statin therapy for primary and secondary prevention in the elderly.6
Statin-associated myopathy (SAM) are part of the therapeutic territory that may be difficult to navigate. While SAM encompasses myalgia, myopathy, and myonecrosis, this discussion will focus on the patient’s perception of myalgia. There are no double-blind placebo-controlled trials nor validated algorithms to circumvent a patient’s poor adherence because they perceive their pain to stem from a statin. Whatever the physician’s perceived prevalence of statin myalgia, what is most important is the patient’s perception of pain and how that perception prevents risk reduction.
There is a perception that statins are bad for “vulnerable” (i.e. elderly) muscle. But statins have been shown to reduce fibrosis and increase muscle force in Duchenne muscular dystrophy. Simvastatin provided a dramatic reduction in inflammation, oxidative stress and fibrosis, resulting in functional improvement.7
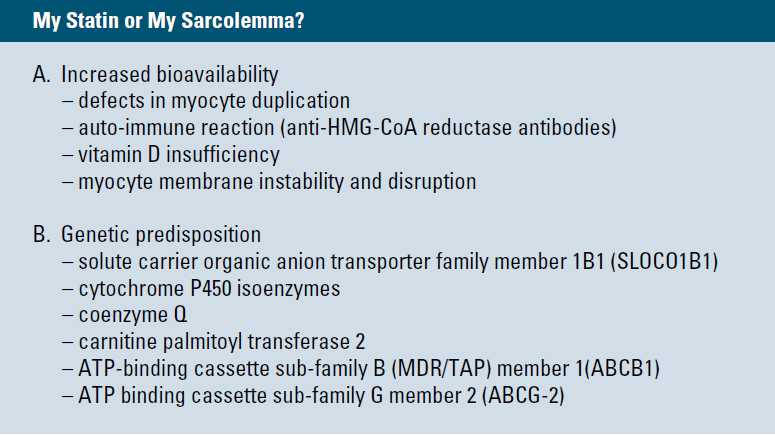
Possible mechanisms responsible for statin intolerance are many and remain a field of active investigation. Peter Toth, MD, recently co-wrote a paper delineating possible contributing factors of myalgia. (Table 1) The most easily addressed issue of statin intolerance may be vitamin D deficiency.
Vitamin D insufficiency doubles when comparing post-menopausal women with those over the age of 65.7 National Health and Nutrition Examination Survey (NHANES) data from 2005–06 revealed vitamin D deficiency, defined as serum 25-hydroxyvitamin D (25OHD) levels <20 ng/ml (50 nmol/L). To convert nmol/L to ng/ml, simply divide by 10 and multiply by four. The overall prevalence rate of vitamin D deficiency was 41.6 percent, with the highest rate seen in African Americans (82.1 percent) followed by Hispanics (69.2 percent). Vitamin D deficiency was associated with lower education, obesity, poor health status, hypertension, lower levels of low-density lipoproteincholesterol (LDL-C), and decreased intake of dairy products. Reasons for this include decreased solar exposure, diet may become less varied with less natural vitamin D, decreased dermal production resulting from atrophic skin changes, and decreased renal production of 1,25 (OH)2D (calcitriol).8
Vitamin D deficiency itself is associated with myalgia.10 The question of whether vitamin D insufficiency contributes to statin-induced myalgia or statins play a causal role in vitamin D deficiency seems to be proven, because atorvastatin has been shown to increase vitamin D levels.
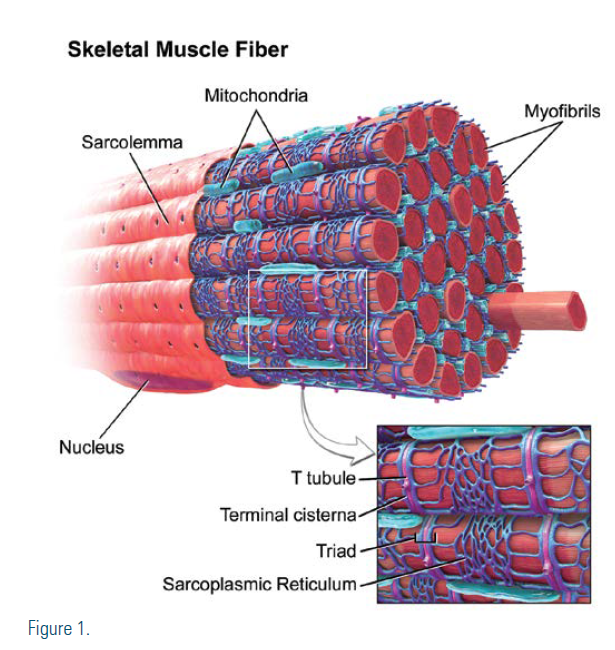
The potential mechanism of vitamin D supplementation on statin-induced myalgia may have to do with direct effects on the sarcolemma and in affecting the metabolism of statins. Vitamin D and vitamin D receptors affect skeletal muscle through genomic and nongenomic mechanisms.13,14 The skeletal muscle contains vitamin D receptors that modulate transcription factors in muscle cells, which in turn mediate cell proliferation and differentiation.15 These affect proteins required for the repair of the T-tubular system and for the prevention of subsarcolemma rupture.16 Vitamin D is responsible for transportation of calcium into the sarcoplasmic reticulum, which is necessary for muscular contraction. Vitamin D is an inducer of Cytochrome P450 3A4 (CYP3A4) and Cytochrome P450 2C9 (CYP2C9), and vitamin D supplementation could reduce the side effects of myalgia by increasing the metabolism of statins and reducing statininduced muscle toxicity. CYP3A4 primarily metabolizes lovastatin, atorvastatin, and simvastatin, while CYP2C9 metabolizes fluvastatin. Pravastatin, rosuvastatin, and pitavastatin are not appreciably metabolized by CYP enzymes.17
A recent study 18 of 146 patients previously intolerant to ≥2 statins had a mean entry vitamin D level of 22 ng/ml and LDL-C of 163 mg/dL. After weekly supplementation, vitamin D levels were normalized to 54 ng/ ml. On re-challenge, mean LDL-C dropped to 88 mg/dL and 91.3 percent of previously statin-intolerant patients were free of SAM. Similar reports have been made.9,19-21
Plasma levels of 25(OH)D should be used to estimate vitamin D status. It may be helpful to recall that 50 nmol/L or 20 ng/ml is needed to prevent rickets and secondary hyperparathyroidism. Current goals may be deemed to be more auspicious. Vitamin D supplementation with 400–2,000 IU/day or 50,000 IU per week is well-tolerated. Three months was the interval used in studies to assess improvement of symptoms and blood levels. As a fat-soluble vitamin, smaller continued doses of vitamin D can often maintain similar levels.
A double-blind study with statin and vitamin D does not currently exist. It may be difficult to find a large enough cohort of patients who are intolerant to ≥2 statins who also are willing to participate in a new study. Until that happens, vitamin D supplementation is a safe, inexpensive, and well-tolerated option for our hypo-vitamin D patients not achieving optimal ASCVD risk reduction because of a perception of statin intolerance.
Disclosure statement: Dr. Stein has no disclosures to report.
Article By:

West County Personalized Medical Care
St. Louis, MO