





.jpg)
.png)










Introduction
In the late 1980s, the Mediterraneanstyle eating pattern received attention after the results of the Lyon Diet Heart Study were published. More recently, the 2013 American College of Cardiology/ American Heart Association (ACC/AHA) Guideline on Lifestyle Management to Reduce Cardiovascular Risk Work Group examined studies involving the Mediterranean-style dietary pattern when developing its diet recommendations, which include: “consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils and nuts; and limits intake of sweets, sugar-sweetened beverages and red meats.”1 The traditional Mediterranean-style eating pattern includes a high consumption of fruits and vegetables; unrefined bread and cereals; potatoes, beans, nuts, and seeds; olive oil or canola oil as the primary fat source; lower-fat dairy products; fatty fish and poultry consumed in low to moderate amounts; eggs consumed less than four times weekly; little red meat consumption; and wine consumed in low to moderate amounts.1-3 Therefore, according to ACC/AHA Guidelines on Lifestyle Management, the Mediterraneanstyle diet is one of several dietary patterns that may be followed by patients to reduce cardiovascular disease (CVD) risk. The challenge has been determining which components of the Mediterranean eating pattern provide its beneficial effects. Research that has examined single components or nutrients of the Mediterranean-style food pattern has failed to support evidence of CVD prevention. More recent research has focused on a Mediterranean Diet (MedDiet) score to determine the association of adherence to the Mediterranean dietary pattern and a decreased risk of CVD risk factors, CVD, and mortality, in general.
Evidence Researchers involved in the European Prospective Study into Cancer and Nutrition (EPIC) evaluated the effect of individual components of the Mediterranean-style eating pattern on all-cause mortality among the Greek cohort (n = 23,349 men and women, not previously diagnosed with cancer, coronary heart disease, or diabetes).4 Adherence to the characteristics of the traditional Mediterranean-style eating pattern was assessed using a 10-point MedDiet scale (range of scores zero to nine, with higher scores indicating greater adherence). A higher MedDiet score (i.e., higher adherence to the eating pattern) was associated with a statistically significant reduction in total mortality. The contribution of the components of the Mediterranean dietary pattern to a lower risk of all-cause mortality in the EPIC study were: higher consumption of alcohol (within the moderate range, 23.5%); lower intake of meat and meat products (16.6%); higher intake of vegetables (16.2%); higher intake of fruits and nuts (11.2%); higher intake of monounsaturated to saturated fat ratio (10.6%); and a higher intake of legumes (9.7%).4
The PREDIMED Study5 — otherwise known as the “Effects of Mediterranean diet on the primary prevention of cardiovascular disease” intervention study — examined whether a Mediterranean diet supplemented with either extra-virgin olive oil (15 liters provided every three months6) or mixed nuts (1,350 g walnuts, 675 g almonds, and 675 g hazelnuts provided every three months6) prevented CVD in 7,447 subjects at high CVD risk. The primary endpoint was the rate of major cardiovascular (CV) events (i.e., cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke). Compared to the control group, the multivariableadjusted hazard ratio for a CV event was 0.70 (95% confidence interval [CI]: 0.54 to 0.92) for the Mediterranean-style diet supplemented with extra-virgin olive oil, and 0.72 (95% CI: 0.54 to 0.96) for the Mediterranean-style diet supplemented with mixed nuts. A point to consider regarding the PREDIMED study is that both Mediterranean-style diet intervention groups received more intense dietitian counseling than the control group, which may have biased the results.7
Overall, a higher adherence to the Mediterranean-style eating pattern has been associated with a decreased risk of multiple CVD risk factors, the metabolic syndrome, and CVD mortality.8,9 The beneficial effects identified in studies are most likely the result of an interaction between the Mediterranean-style eating pattern components versus a single food group.8 The specific CVD risk factors that have been associated with the Mediterranean-style eating pattern include improvements in blood lipid levels and particle size, reductions in blood pressure, decreased insulin resistance, improved glucose control, improved antiinflammatory markers, and a decreased risk of stroke.8,9 The substantially reduced risk of CVD associated with Mediterraneanstyle dietary patterns has been found in the absence of weight gain.2,10
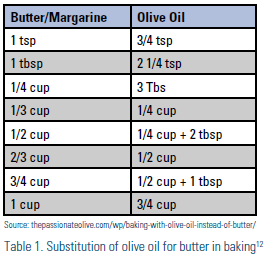
Practical Applications An important point to emphasize to patients is that the Mediterranean-style eating pattern is not simply a matter of using extra-virgin olive oil instead of butter — it is a lifestyle. Practitioners should advise and encourage patients to embrace the traditional Mediterranean style of living. Lifestyle habits that typically accompany and may contribute to the beneficial effects of the traditional Mediterranean-style eating pattern are daily physical activity; awareness of portion sizes and eating mindfully (i.e. awareness of physical cues of hunger and satiety, and using all of the senses in choosing to eat food that is both satisfying and nourishing11); meals in the company of others; maintaining or achieving a healthy body weight; and moderation as an overall lifestyle approach. Switching to the Mediterranean-style eating pattern may seem overwhelming to some patients. Patients should be encouraged to choose one or two of the Mediterranean-style eating pattern components to add to their current eating habits. Simple suggestions to offer to patients are included in the tear sheet of this LipidSpin and may include using extra-virgin olive oil in food preparation (see Table 1 for substitution of olive oil for butter in baking); using avocado instead of butter, cream cheese, and mayonnaise; eating 1 ounce of nuts and/or nut butter each day; and focusing on mindful eating and flavorful cooking (go to oldwayspt.org/recipes for ideas). For personalizing patients’ cardio-protective dietary patterns, consider referral to a registered dietitian nutritionist (RDN).1
Disclosure statement: There are no disclosures to report.
References are listed on page 36.
Article By:

Idaho State University
Kasiska School of Health Professions Coordinator, Cardiovascular Risk Management Clinic Pocatello Cardiology
Diplomate, Accreditation Council of Clinical Lipidology

University of California Irvine Preventive Cardiology Program
Associate Clinical Professor of Medicine (Cardiology)
University of California Irvine School of Medicine
Diplomate, Accreditation Council of Clinical Lipidology