





.jpg)
.png)










I love the theme of this edition of the LipidSpin, Lipids & Aging. When you read through the various articles, you will find outstanding discussions regarding the many aspects of treating older patients. Whenever I treat older patients with dyslipidemia, I always start by considering the overall risks versus benefits of statin therapy. Then I proceed to other aspects and considerations of providing patient-centered care. One aspect that is considered by many is the potential for “polypharmacy.”
The term “polypharmacy” has a negative connotation when associated with the elderly. It implies the prescribing of medications that are unnecessary, exposing patients to unnecessary risks related to side effects, increasing risk of potentially dangerous drug-drug interactions, and increasing costs of medications. However, many of these considerations can be rebutted with evidence. The literature describing safety and efficacy of statin therapy is continually updated with new analyses of evidence that provide an overall supporting message.1 Additionally, the American Heart Association recently published a statement titled, “Recommendations for Management of Clinically Significant Drug-Drug Interactions with Statins and Select Agents Used in Patients with Cardiovascular Disease: A Scientific Statement From the American Heart Association,” which provides recommendations for managing significant drug-drug interactions with statins.2 This scientific statement should be used to assist clinicians in the effective and safe prescribing of statin therapy. However, an additional element that is relevant to our older patients is the cost of therapy.
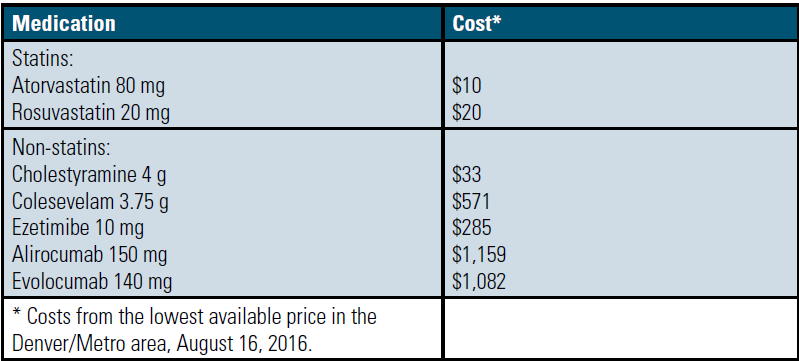
Statin-based therapy is comprised of multiple generic options. Most commercially available statin medications are available generically, including both high-intensity statin options, atorvastatin and rosuvastatin. Therefore, the cost of statin therapy can be as low as a generic copay for your elderly patients. Elderly patients, many of whom have fixed incomes, may have a difficult time paying for high cost brand-name only medications, even if they have a favorable brand-name copay. For patients who purchase their medications outside of their insurance, Table 1 provides a cost comparison of LDL-C lipid-lowering medications using GoodRx.com. This website provides estimates of the cost of medications, which typically are the lowest prices available in your geographic area when you use the printable coupon (please see the website for specific instructions and restrictions). Comparatively, statin therapy is much more affordable than other options.
On the horizon is generic ezetimibe. The first generic version of this medication is due to be available in December 2016. However, when a brand-name only medication becomes a generic, the price of the first generic version is typically just a little lower than the brand-name price. We saw this happen with atorvastatin, and then again with rosuvastatin earlier this year. This is because usually only one manufacturer is granted exclusive rights for the first generic distribution of a medication for a period of about six months. After that period of exclusivity ends, multiple manufacturers are authorized to distribute their generic versions. When that happens, the prices usually drop significantly.
It is a privilege to be the co-editor of LipidSpin. I hope you enjoy this edition as much as I have!
Article By:

Professor, Clinical Pharmacy and Family Medicine
University of Colorado Denver
Anschutz Medical Campus
Aurora, CO
Diplomate, Accreditation Council for Clinical Lipidology